Schroth Method for Kyphosis
So many of our patients walk into their first visit with us saying, “I’m here because I’ve seen those little old ladies hunched over their walkers, and I don’t want to be one of them.” The medical term for what they are referring to is kyphosis.
Kyphosis is most often associated with the thoracic spine, or mid-back, although it can happen pathologically in any section of the spine – more on that in a future post.
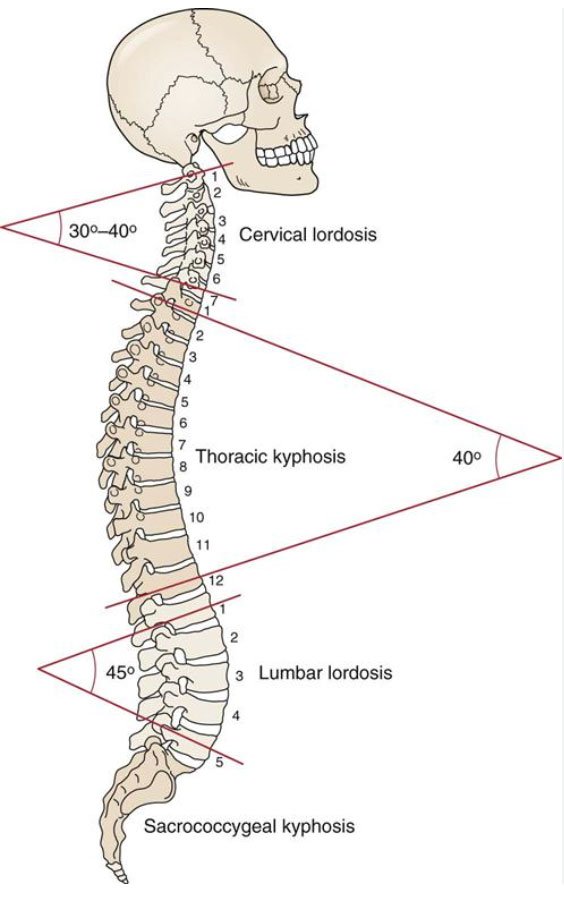
Normal Sagittal Curvature of the Spine
Understanding the term kyphosis is nuanced, as the thoracic spine naturally has kyphosis, which means a forward rounding. When most healthcare professionals throw around the term kyphosis, what they actually mean is that an individual has excessive kyphosis.
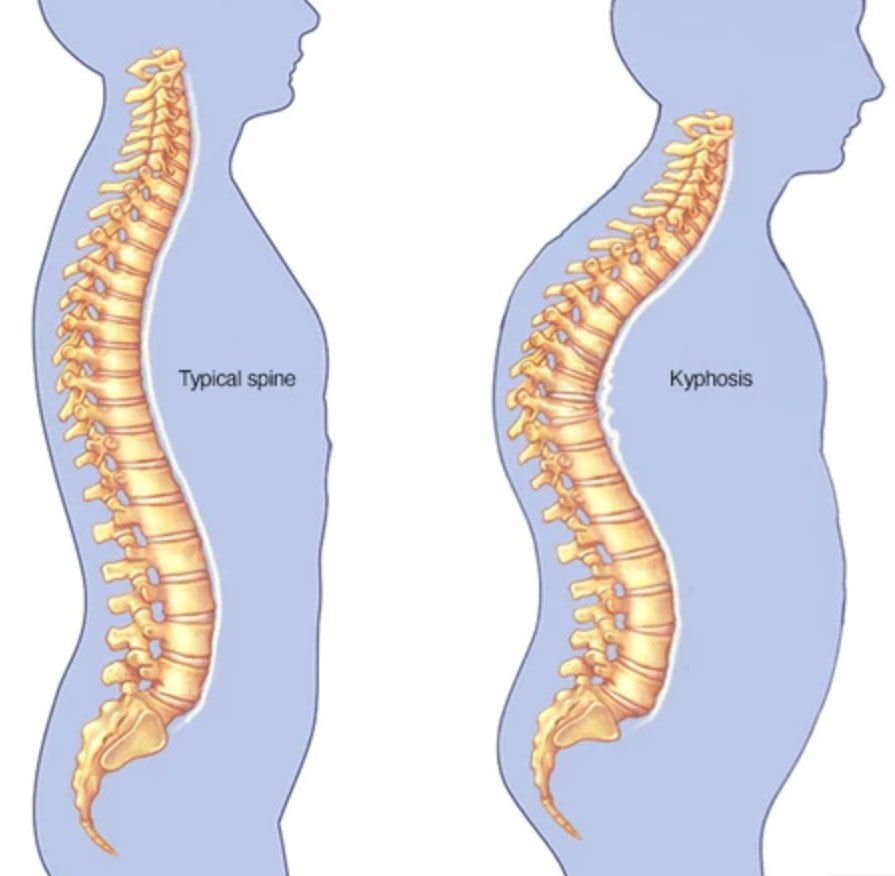
Typical vs Excessive Kyphosis
Functional Versus Structural Kyphosis
There are 2 types of kyphosis, and it’s important to know the difference – for both healthcare professionals and patients. It will inform your choice of treatment.
Functional Kyphosis
Functional kyphosis is a function of something else – most typically hypermobility (i.e. laxity) in the joints and weak postural muscles. These are individuals whose bodies are comparable to Gumby, the beloved cartoon character, known for his bendiness and flexibility.

Gumby
These folks lack an appropriate amount of stiffness in their spinal joints, and can easily collapse into a very rounded spinal posture. (They also will often be able to do “party tricks” like put their feet behind their heads, bend their pinky fingers all the way back to their forearms, and many more. All of their joints are hyperflexible. To read up on hypermobility syndromes, check out this previous blog post Hypermobility and Scoliosis.
Hypermobile people have to work much harder to strength train their postural muscles – without structural stability, they must rely on their spinal muscles to hold them upright. Unfortunately, most hypermobile people don’t know this and therefore have undertrained/underdeveloped spinal muscles.
Another interesting element of functional kyphosis: the psychological component. Human posture is a reflection of our attitudes, and how we’re feeling. When we are sick, tired, and stressed, we are more likely to be showing up in the world kyphotic.

Typical Teenage Functional Kyphosis
Additionally, when we lack confidence, want to be invisible, or are going through puberty changes like breast development, kyphosis shows up. The connection between mind and body profoundly impacts our spinal positioning.
Alternatively, when we are feeling well, energized, and confident, our spines reflect that – we stand taller, spines long, more open in the heart space and the front of the body.

Thriving Posture
Structural Kyphosis
Next up, is structural scoliosis. This type involves actual bony deformation of the vertebrae. Scheuermann’s Disease, also called juvenile kyphosis, is one of the widely known types of structural kyphosis. A phenomenon called anterior wedging occurs in at least 3 or more adjacent vertebra.

Anterior Wedging
This bony change in the vertebrae causes the spine to change shape; to become more curved, more kyphotic.

Schuermann’s Disease
We know a kyphosis is structural when the person bends forward during the Adams Forward Bend Test and the thoracic spine becomes even more kyphotic.

Structural Kyphosis During Adams Forward Bend Test
Another common cause of structural kyphosis is due to osteoporotic fractures in the spine. When bone density in the vertebra is low, microfracturing can occur, causing the vertebra to lose height, especially in the anterior half. Once again, the “wedging” of the anterior half of the vertebra causes flexion, or rounding of the spine.

Osteoporotic Kyphosis
Sadly, this is the type of kyphosis that our patients are referring to they talk about “the hunched over the walker” posture. This type of kyphosis can be easily prevented – one who is diagnosed with osteopenia or osteoporosis should immediately seek out postural physical therapy, like Schroth, in order to learn how to prevent fracturing from occurring.
Prevention involves postural exercises, as well as using movement patterns that alleviate pressure from the anterior vertebrae (e.g. hip hinging, spinal elongation, stretching the pectorals).
One key difference to understanding functional vs. structural kyphosis, and implications for treatment:
FUNCTIONAL = FLEXIBLE
STRUCTURAL = STIFF
Functional kyphosis is easily reversible
Treatment involves educating the patient about their kyphotic spinal position – by showing them photos of themselves and using mirrors in front of them and to the side of them. Once they understand how they are showing up in the world (oftentimes they are mortified – they didn’t realize how hunched they are), we teach them how to change their posture by using their spinal muscles.
The Schroth Method can make a profound difference on a functional kyphosis. Body awareness, spinal elongation, and proper breathing, all happen together to contribute to an improved posture of the spine.
Structural kyphosis is not quite a simple
Because of the stiffness of the kyphosis, the person cannot easily elongate and grow taller like a person with functional kyphosis can. It proves much harder to reverse. BUT, Schroth Method to the rescue once again.
We have a secret weapon called bilateral shoulder traction, a special and specific way to activate the upper torso muscles. This type of muscle activation sets off a chain reaction: it opens up space in the chest in order for the vertebrae to begin to move anteriorly, which straightens the thoracic spine.

Schroth Method: Bilateral Shoulder Traction
Expansive breathing and axial elongation, cornerstones of the Schroth Method, are applied with bilateral shoulder traction, and the result is a lessened kyphosis.
Whether you have a hypermobility syndrome causing your scoliosis, or Scheuermann’s Disease, or osteoporotic kyphosis, take some time to learn about your body. Understanding the origin is your guide to selecting treatment. We hope to see you in the clinic soon.