Treating Adult Scoliosis with the Schroth Method
Adult scoliosis is surprisingly prevalent in our population. There are three types: Adult-onset, also known as De Novo Scoliosis, Progressing or Stable Adolescent Idiopathic Scoliosis, and Secondary Scoliosis.
Adult-onset or De Novo Scoliosis affects up to 70% of our elderly population and is the most common type of older-adult scoliosis that we see at SchrothDC. This is a degenerative type of scoliosis that starts later in life. It is mostly due to disc changes and facet joint arthritis happening asymmetrically in the spine. This type of curvature occurs most often in the lumbar or the thoracolumbar spine. Back pain and other spinal symptoms, such as stenosis, often accompany this type of scoliosis (an important distinction from Stable Adolescent Idiopathic Scoliosis.)
Adult scoliosis progression can be unpredictable. However, as a general rule of thumb, we expect De Novo curves under 30 degrees to progress about .5 - .75 degrees per year, and curves between 31-50 degrees to progress about 1 degree per year. In large curves, meaning those over 60 degrees, there can be severe collapse during the course of a day due to gravity, of up to 20 degrees (meaning your 60 degree curve upon waking could be an 80 degree curve by the time you’re getting ready for bed).
Our second type of adult scoliosis are the folks who were diagnosed in adolescence, and have been living with it since then. Stable Adolescent Scoliosis seen in adulthood (we mostly see this in our 20, 30 and 40 year old patients) is not nearly as often accompanied by pain and back symptoms. Adolescent-onset scoliosis can be progressive when combined with degenerative factors as discussed above – we see this mainly in our patients > 50 years old. These curves will also often progress (in women) during and after menopause, when changes in muscle mass and bone density occur.
The third type of adult scoliosis we see is called Secondary Scoliosis, meaning it is secondary, or due to another factor, such as bony abnormalities like leg length discrepancy, pelvis obliquity, or asymmetrical anomalies at the lumbosacral junction. It can also happen in conjuction with hip pathology or post-surgically – it’s very common after spine laminectomies. An extremely common culprit is osteoporosis, which means low bone density, and the associated vertebral fractures that happen with this disease. Lastly, secondary scoliosis could be neuromuscular in origin, in those who have spinal cord injury, Osteogenesis Imperfecta, Cerebral Palsy, Spina Bifida, Muscular Dystrophy, and Polio.
Knowing the origin of one’s adult scoliosis is imperative in choosing the best physical therapy treatment for that individual. As a therapist, treating a Stable Adolescent Idiopathic Scoliosis in a 30-year-old will be radically different from treating a De Novo scoliosis in a 70 year-old-patient. The beauty of the Schroth Method is that it is adaptable to all populations.
Before we begin treatment with any adult, we look at a recent x-ray of the entire spine. We are mainly looking for what I will call “sensitive areas” – in medical jargon, spondylolisthesis. These are areas that need to be protected and stabilized. We take extra precautions when treating those with spondylolisthesis. Over-stretching and focusing on mobility rather than stability in these areas are the worst thing for them, and the patient will likely not make long-term progress if focusing on these things.
We are also hyper-interested in the Sagittal alignment of the spine, which is the view from the side (our profile).
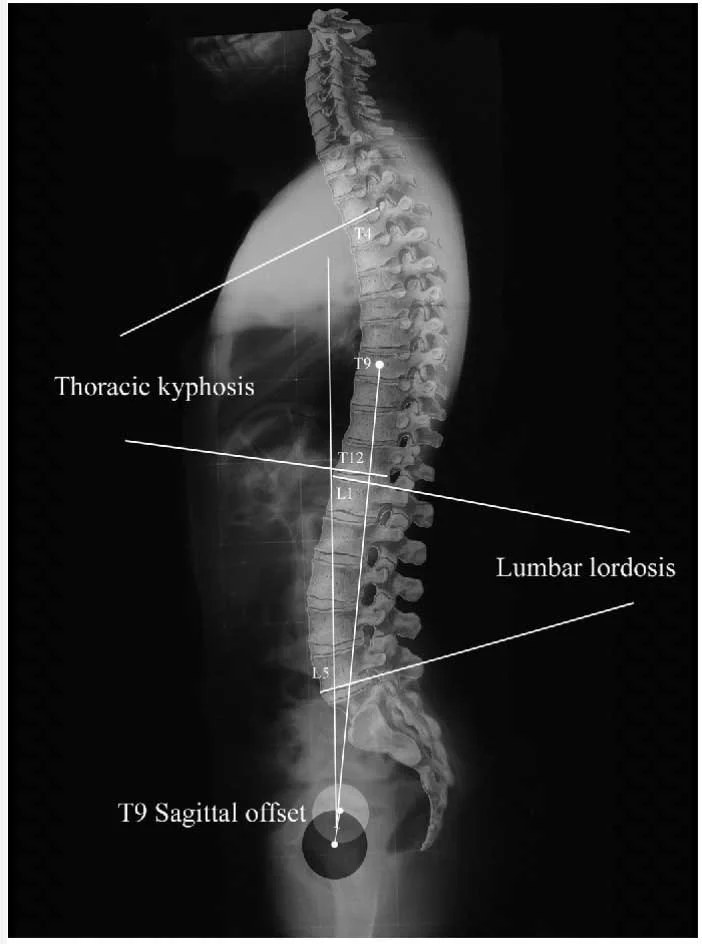
Normal Sagittal Plane Alignment
One’s sagittal alignment, and the preservation of the natural lordoses and kyphoses of the spine, is the biggest predictor of whether they will experience pain, and therefore is a significant focus of adult scoliosis treatment. When we see a loss of lumbar lordosis, a thoracolumbar kyphosis, or a loss of cervical lordosis, we know we need to focus on restoring the sagittal plane parameters with the patient.
Once we have gathered the needed information from the patient’s x-ray, we develop a treatment plan, based both on our findings and on the patient’s goals.
The Schroth Method will always include axial elongation, or stretching oneself upward against gravity, diaphragmatic breathing, and symmetrical weight bearing postural exercises.

Katharina Schroth working with adult patient
Additional exercises will vary from patient to patient: our stiff patients will need additional stretching and mobility exercises, for example; stretching of the pectoral muscles, the hamstrings, the hip flexors, or mobilization of the thoracic spine and ribcage. Our hypermobile (hyperflexible) patients will need exercises that focus on spinal and core stability, such as bird dog and dead bug. Some patients will need exercises to help improve balance and gait.
Patients coming to us who are symptomatic may need manual therapy intervention, such as joint manipulation, deep tissue massage, or dry needling. This can alleviate pain and allow the patient to progress through the exercises more comfortably.
Setting realistic goals and expectations in any type of physical therapy is key. It’s important to note here that the Schroth Method looks very different when utilized with teenagers than when used with adults. If you’ve visited our website and you’ve seen those mesmerizing “before and after” photos, of course you’re coming to us excited about changing the appearance of your torso. We really need a disclaimer below some of those photos stating that the most dramatic changes you see are in bodies who are skeletally immature, in those who are aged 10-14. We cannot and do not expect the extreme torso re-shaping we see in an 11-year-old to occur in a skeletally mature adult, sadly. The spine, as well as all of our tissues in our bodies, stiffens and settles into place with each passing year. It would be false advertising to tell any adult that the Schroth Method can straighten their spine, as much as I would like it to.
The main goal of applying the Schroth Method to adult scoliosis is to prevent progression of the scoliosis, which is a big deal. Preventing .5 - 1 degree of progression from happening with each passing year, could likely curtail future pain and other back symptoms. We also hope to strengthen the core muscles and alleviate pain and symptoms related to the spine.
Empowering patients to take care of their backs, and giving them research-based tools in order to do that, is always our number one goal at SchrothDC. At the risk of sounding like your parents (no matter how old you are) “you only get one spine”, so please, take care of it.