Foundations of The Schroth Method
Happy almost-fall folks. Take a look around, what do you see? Are you noticing the tips of the trees turning reds and yellows? Can you hear the crunch of the already fallen leaves under your feet? Feel the quality of the air around you – can you distinguish it from our humid DC summer air?
Many of us humans move through life at breakneck speed – we have demanding jobs, we have spouses, kids, pets; houses to keep clean, maybe even aging parents we’re taking care of. All of these obligations take up A LOT of headspace. We often miss the small details unfolding around us.
How does this tie into the Schroth Method? What I’m describing above is called awareness. (The popular buzzword for this is Mindfulness.) The Schroth Method requires a great deal of awareness; more specifically, it requires a great deal of body awareness.
Body Awareness
Body awareness, known scientifically as proprioception, is a skill that we are born with. et some people’s proprioception is much sharper than others. (Sidenote: Did you know the 2021 Medicine Nobel Prize was awarded to David Julius and Ardem Patapoutian for their discoveries in proprioception?)
We’re not entirely sure why some people have a strong sense of proprioception and others don’t. Perhaps it’s genetic, or psychologically influenced, or a combination of both. The good news is, we can cultivate body awareness; meaning, we can get better at it with practice.
During our 1st visit with patients, called an Initial Evaluation, we assess each patient’s body awareness by asking them specific questions about their body position. Our clinic is practically wallpapered with mirrors, so patients are getting near-constant visual feedback about their bodies. We will also ask patients to close their eyes on occasion so that they can feel asymmetries in their bodies versus solely seeing them.
It's very easy to tell who has great body awareness versus who is lacking body awareness. Those with great body awareness will advance more quickly in the Schroth repertoire. Those without, will need to build their proprioception skills as they are beginning a Schroth program – but remember, proprioception can be learned - so these folks can still be successful with Schroth.
Once we assess body awareness, we begin to teach the principles of Schroth postural correction.
Rooting Downwards
All of us need a stable base to ground our bodies to the earth. It is only from this grounding down that we can grow upward.
Scoliotic curvature of the spine very often pulls the entire torso over to one side – the side of the dominant curve. This pulling means that our weight shifts from being symmetrical, or 50/50 through the lower limbs, to being asymmetrical.

In sitting, we ask our patients with scoliosis, “Are you sitting more on one hip, or one SITS bone than the other?” Those with good proprioception can identify this, correctly, immediately. Those without good proprioception will say things like “I’m not sure”, or “Maybe the left?”
In standing, we ask “Are you standing on one foot more than the other?”
Once we establish the specifics of the asymmetry, e.g. “you’re sitting more on your left hip, because your dominant curve is on the left” - we teach our patients to root down evenly through the hips (in sitting) and in the feet (in standing).
3-Dimensional Postural Correction
Rooting downward is the first step of what we call 3-D Posture Correction in Schroth. Scoliosis is a 3-dimensional dysfunction and therefore requires a 3-dimensional solution. The 3 planes of motion are sagittal, coronal, and transverse. When first teaching Schroth, we break postural corrections into their individual components.
With training and practice, patients can eventually do all of their corrections at once, almost as if the correction is becoming an art form rather than a science. This process is known as torso-reshaping. The following sub-principles are all part of 3-D Postural Correction.
Pelvis Corrections
The pelvis, made up of the 2 hip joints and the sacrum, is the base or foundation of the spine. The feet need to be our stable base for our pelvis, and the pelvis needs to be a stable base for our spine. Scoliosis alters the position of the pelvis in all 3 planes of motion. Any malalignment of the pelvis can affect the posturing of the spine.
We aim to make pelvis corrections in the sagittal plane first, then in the coronal plane, and finally in the transverse plane. Our goal is to achieve the most neutral position of the pelvis, then we can move on to spinal re-alignment.
Elongation
Once we root downward through the hips or feet evenly and make our pelvis corrections, we can begin the process of spinal elongation, also called axial elongation. This involves contraction of the erector spinae muscles to quite literally “erect” the spine.
We will often use imagery such as “grow tall like a tree”, or “imagine your head is being pulled upward toward the sky”. Tactile cueing, such as applying gentle pressure to the top of the head and instructing the patient to “push into my hand” is also effective in achieving spinal elongation.
Active elongation of the spine is the act of resisting gravity. The gravitational force on our planet is pushing down on our heads and spines, causing vertebral compression, slumped posture, and worsening of scoliosis (if present). Our ability to elongate our spines throughout our lives will dictate how upright our spines stay.
It’s important to note here that spinal elongation is active. People ask me all the time if inversion tables are good for scoliosis. Strapping your ankles into an inversion table and spinning yourself upside down is a passive therapy – it requires no effort of the spinal muscles to erect the spine.
In other words, you could sleep upside down every night on your inversion table, but if you’re not activating your spinal muscles against gravity during the day while sitting and standing, your back will be weak and your posture will be poor.
Expansion
There are two principles of expansion in the Schroth repertoire. The first is called shoulder traction, which is the act of reaching outward through the shoulders and elbows during postural correction. This exerts an east-west (or horizontal) tension on the ribs and indirectly the spine, to help with spinal straightening and opening the scoliotic concavities.
The second is the style of breathing we use during Schroth exercises, which involves 360° expansion of the ribcage. This is an extremely active breathing technique, during which we use the diaphragm and intercostal muscles to push the ribcage outward in all directions during the inhalation, and hold the ribcage outward on the exhalation.
This last part can be very challenging, as eccentrically contracting the diaphragm and intercostal muscles is unnatural. Most patients need a lot of practice with expansive breathing before feeling confident they are doing it correctly.
Here’s a pro-tip from Eric Campesi: SLOW DOWN the breath, especially the exhalation. It will give you time to think about what’s needed to maintain your expansion.
Muscle activation
The expansion technique is a segway into the next principle, which is called Muscle Activation. Muscle activation is the ability to maintain the expansion of the scoliotic concavities and prevent the collapses of the torso that scoliosis causes. Muscle activation at its most extreme can involve pushing long wooden dowels, also called Schroth Poles, into the ground or wall during exercise.
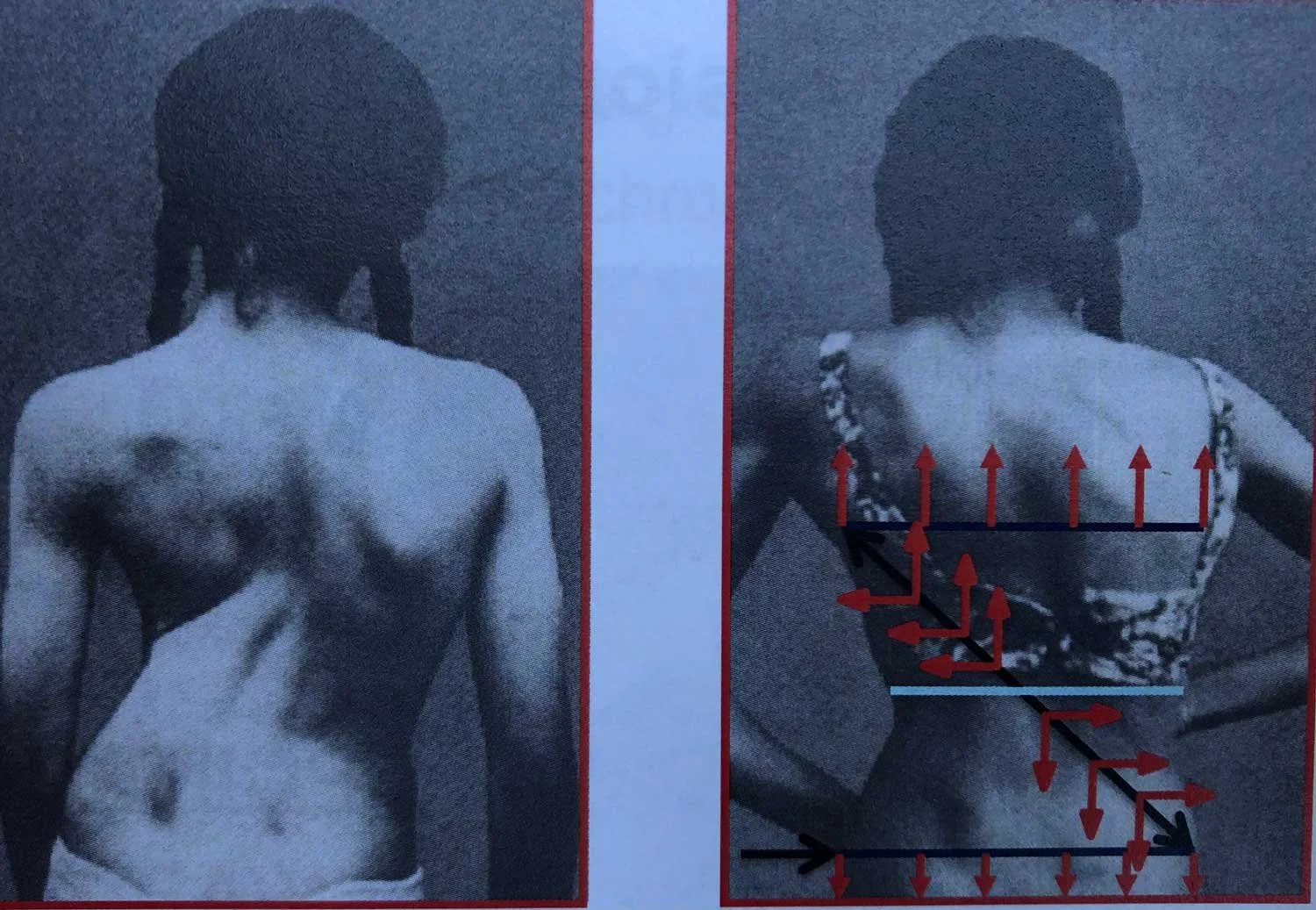
3-D Postural correction with expansion technique
Trunk Symmetry

Trunk imbalance
By the time we are this far along in our Schroth exercise, we should be achieving what’s called Trunk Symmetry. Trunk Symmetry is altered by scoliosis – the dominant scoliotic curvature pulls the torso to one side, creating a trunk imbalance.
The side of the trunk with the primary scoliosis is “larger” than the other side of the trunk when divided down the middle. Trunk symmetry also speaks to the head being centered on top of the pelvis – another piece of alignment affected by scoliosis.
Through Schroth, we have the ability to restore trunk symmetry, by engaging in the principles above.
If your head is spinning, we admit, the Schroth methodology is undoubtedly complex. The research that has been done on learning Schroth concluded that patients need a minimum of 10 hours of 1:1 Schroth instruction in order to feel proficient and confident in the exercises.
We feel honored to serve as guides for every patient that walks through the doors of SchrothDC. We pride ourselves on being thorough and treating every patient as an individual. There are no cookie-cutter treatment plans offered at SchrothDC, only bespoke, thoughtful, Schroth therapy. We hope to see you in our clinic soon!